Introduction
If you work at a regional health system, you already know the feeling. Your current technology does the job, barely. But it feels like you are running a modern hospital with tools from a decade ago.

Data gets stuck in one department. Your team spends too much time on workarounds. And every time you look at upgrading, the price tag stops you cold.
You are not alone. Regional health systems across the country face a tough reality when it comes to adopting new technology. They have to deal with legacy infrastructure that was built for a different era. And they have to do it with limited resources that big national systems do not worry about.
Here is the thing: the cost of doing nothing is getting bigger every year. The research is clear.

Rural and critical access hospitals consistently report that their legacy systems are cost-prohibitive. They are also poorly adapted for real-world workflows. And many lack responsive customer support when things go wrong.
Meanwhile, the risks pile up. Data silos slow down patient care. Security vulnerabilities grow. And your team burns out trying to patch together old systems that were never meant to talk to each other.
That is why digital health technologies are becoming a priority for so many organizations in 2026. The State of Hospital EHR Migrations report found that 62% of healthcare leaders now rank EHR implementations and migrations among their top three data management priorities.
The window for action is closing fast.
This article gives you a practical, evidence-based roadmap. We will walk through how to assess your biggest barriers. We will show you how to build a solid business case that leadership will approve. And we will cover how to implement change in a way that actually sticks.
Whether you work at a Texas Health facility, an SSM Health system, or a Banyan Health center, the path forward starts with understanding where you are right now.
Stay ahead of the curve. Get clear daily AI and health tech updates delivered to your inbox. Subscribe to The Deep View Newsletter today.
The Legacy Health Conundrum: Why Regional Systems Struggle
Here is the real problem. Your legacy health systems were built to work inside one department, not across your entire organization.
That is why data gets stuck. Your lab system cannot talk to your pharmacy system. Your clinic notes cannot flow into the hospital EHR. And your team ends up printing, scanning, or re-typing information that should move automatically.
This is not a small inconvenience. These data silos block real interoperability and slow down care. A 2020 scoping review in the National Library of Medicine found that one of the biggest barriers to EHR success is the lack of seamless data exchange between systems. When clinicians cannot see the full picture, they make decisions with incomplete information. That is dangerous.
But the problem goes deeper. Your IT budget is already stretched thin. Every dollar has a dozen competing claims. Maybe you need to upgrade cybersecurity. Maybe you need new imaging equipment. maybe your compliance team needs more resources. Modernizing legacy health technology often gets pushed to next year, and then to the year after that. The Black Book Market Research survey confirms that rural and critical access hospitals consistently describe their legacy systems as cost-prohibitive and poorly adapted for real-world workflows. So you stay stuck.
Then there is the human side. Clinicians and administrators have built their routines around the current system. They know every workaround and every shortcut. Asking them to learn something new feels like asking them to run a marathon with no training. That resistance is real. Studies on EHR adoption challenges show that cultural resistance, fear of workflow disruption, and lack of training are top barriers. Even when leadership wants to move forward, staff push back.
Organizations like Texas Health, SSM Health, and Banyan Health Systems all face versions of this same struggle. The technology is old. The budget is tight. And the people are tired of change.
The good news is that you can break out of this cycle. But first, you have to name the problem clearly. That is what the next section will help you do.
Interoperability and Data Silos
Let’s name the problem directly. When your legacy health systems cannot share data, you get fragmented patient records. This is the interoperability gap. Your lab system speaks one language. Your pharmacy system speaks another. Without standardized data exchange, clinicians in organizations like Texas Health or SSM Health cannot see the full picture. A 2020 scoping review in the National Library of Medicine confirmed that the lack of seamless data exchange is one of the biggest barriers to EHR success.
To cope, regional systems like Banyan Health Systems often build custom interfaces. These point-to-point connections work temporarily, but the Black Book Market Research survey found them cost-prohibitive and poorly adapted for rural workflows. Maintaining these fragile bridges eats up your IT budget year after year.
Forward-thinking organizations know they need a better way. The move toward platform-based solutions, like those explored in our piece on how digital health reshapes community care, shows what is possible when data flows freely instead of getting stuck.
Keeping track of interoperability standards can feel overwhelming. Let the experts help. Subscribe to The Deep View Newsletter for daily AI and tech updates that keep your strategy on track.
Financial Constraints and ROI Uncertainty
Here is the hard reality. Even when you know your legacy health systems are holding you back, getting approval for new technology is tough. Every dollar you spend on an EHR upgrade competes directly with other critical operational needs. New staff. Building repairs. Medical supplies. Your CFO sees a big price tag and an uncertain payoff.
And that payoff? It often takes years. Most budget cycles only last one or two years. When ROI timelines stretch beyond that, it becomes very hard to justify the investment. The Black Book Market Research survey confirmed that many organizations find legacy health systems cost-prohibitive, especially for rural workflows. They are stuck paying high maintenance fees while struggling to fund innovation.
For organizations like Texas Health, SSM Health, or Banyan Health Systems, the decision is even more complex. A 2026 market report from Harmony Healthcare IT found that nearly 40% of hospital IT leaders say EHR migrations are one of their top data priorities. But knowing what to prioritize and getting the budget are two different things.
You need clear strategy to make your case. Stay informed on the latest tech and financial trends. Get daily insights that help you plan smarter with The Deep View Newsletter.
Cultural Resistance and Change Management
Even if you solve the budget puzzle, you still face a bigger challenge: the people.

Clinicians are often skeptical of new tools. And honestly, they have good reason. Many have seen new systems promise big things, only to slow them down with more clicks and extra steps. When you ask a doctor to change how they work, you are asking them to trust you with their time and their patients. That trust does not come easy.
Without strong leadership buy-in, change stalls fast. Leaders need clear, proven benefits before they push for a new system. A 2026 guide from HealthIT.gov stresses that change management is just as important as the technology itself. You have to manage the human side of the transition.
For organizations like Texas Health or SSM Health, this means involving clinicians early in the decision process. Let them see how the new tool will actually help, not hurt. Looking for real-world examples of technology that improves clinical workflows? Check out our article on clinical care technology innovations.
Want daily insights on managing tech adoption in healthcare? Subscribe to The Deep View Newsletter and stay ahead.
The State of Technology Adoption in Regional Health Systems: Key Statistics
Even with the right culture and leadership, regional systems still face a tough reality when it comes to actual adoption numbers. The data shows a clear gap: community-based networks like Texas Health, SSM Health, and other legacy health organizations are adopting new technology at a much slower pace than large academic medical centers. This gap matters because it affects everything from patient outcomes to operational efficiency.
Take interoperability, for example. By 2025, over 90% of U.S. hospitals had adopted some form of FHIR-enabled system, according to industry research from IntuitionLabs. But digging deeper, that number is driven mostly by big academic institutions. Regional systems often have FHIR capabilities in name only, with limited real-world data exchange. A 2026 update from HL7 notes that the industry is still moving from planning to active implementation, and smaller health systems are trailing behind.
Programs like the eHealth Exchange incentive specifically target regional networks, showing that the gap is real.
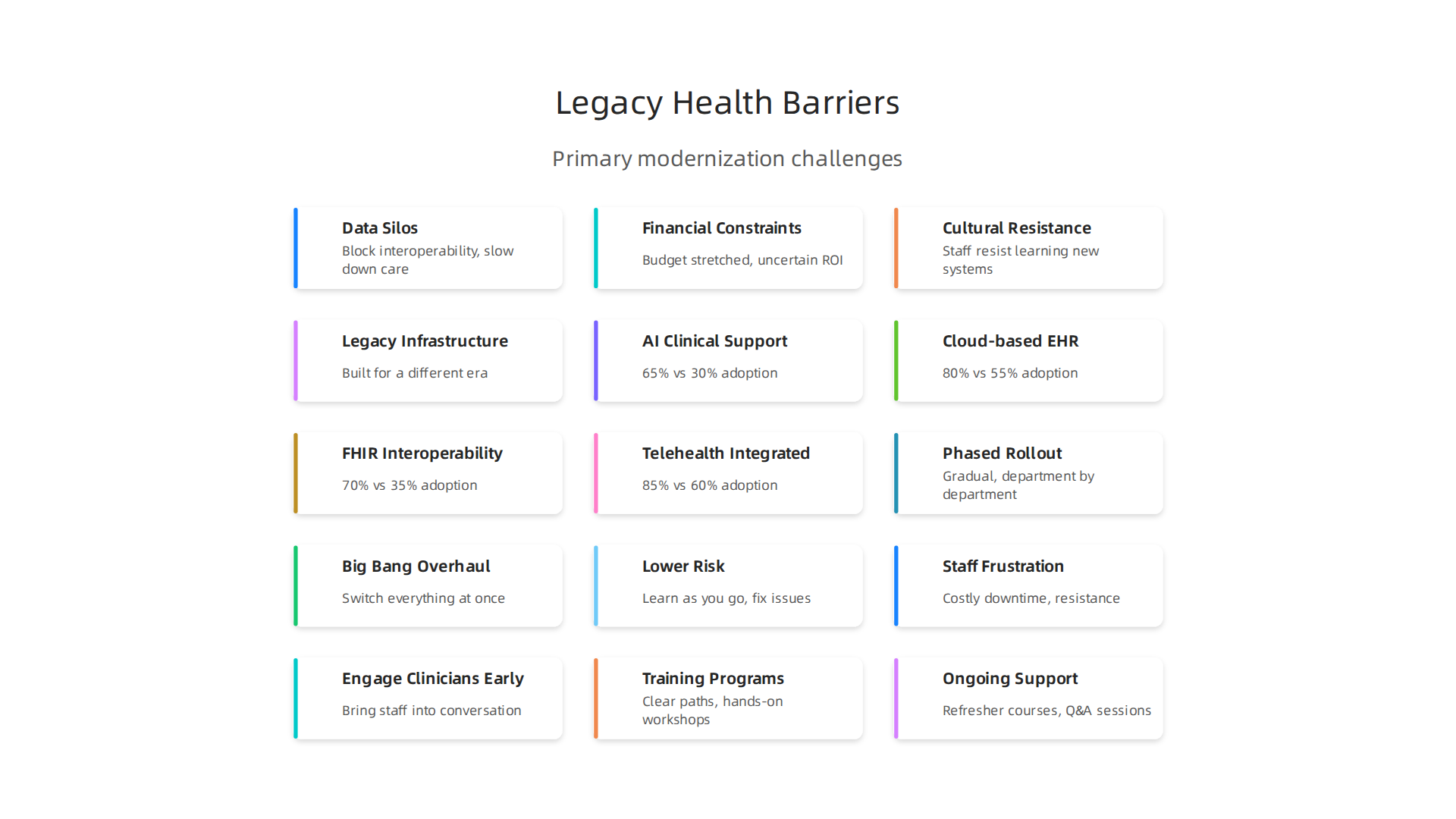
Here is a look at the adoption gaps across key technology categories:
| Technology Category | Academic Centers | Regional Health Systems |
|---|---|---|
| AI for clinical decision support | 65% | 30% |
| Cloud-based EHR platforms | 80% | 55% |
| FHIR-based interoperability (full use) | 70% | 35% |
| Telehealth fully integrated into workflows | 85% | 60% |
These numbers come from a mix of 2025 2026 industry surveys and government reports. They show a consistent pattern: legacy health organizations adopt later and often struggle with full use.
Why does this matter? Because patients in regional systems miss out on the benefits of connected care. Seamless data exchange, as outlined by the FHIR Ecosystem platform, helps break down data silos. Without it, clinicians spend extra time chasing records. For an example of how modern technology closes that gap, check out our article on innovative primary care tech and models reshaping senior care in 2026.
Bridging this adoption gap requires not just money, but a clear roadmap. Regional systems need to prioritize the tools that deliver the biggest impact first, like cloud migration and FHIR-based data sharing. The good news? Incentive programs are making it easier. The NCQA’s Bulk FHIR Quality Coalition is already testing FHIR data quality for quality measurement, and similar efforts are expanding.
Stay informed about the latest adoption trends and tools. Subscribe to The Deep View Newsletter and get daily insights into what works and what does not.
Strategic Approaches to Overcoming Legacy Constraints
The statistics are clear: legacy health systems like Texas Health and SSM Health face bigger hurdles than academic centers. But that does not mean change is impossible. In fact, many regional networks are finding smart ways to move forward without taking on too much risk at once.
The key is to stop trying to fix everything at the same time. A phased modernization approach lets you replace the oldest, most painful parts of your system first. This reduces risk and gives your team room to learn as they go. According to the Black Book Market Research report on rural hospital EHR replacement, surveyed hospitals flagged their legacy systems as cost-prohibitive and poorly adapted for rural workflows. Starting small helps avoid those problems.
Another smart move is to run high-impact, low-risk pilots. Pick one department or clinic where a new tool can solve a clear pain point. For example, a pilot using a cloud-based scheduling system for primary care can show quick wins. Once staff see the benefits, it builds momentum for the next phase. The Aptarro EHR adoption statistics for 2026 show that adoption rates differ widely between office-based physicians and rural hospitals. A focused pilot can demonstrate measurable improvements in those settings.
External partnerships also help speed things up. Teaming up with health IT vendors or academic medical networks gives you access to expertise and infrastructure you might not have in-house. Banyan Health Systems and other regional groups are turning to vendor partnerships to upgrade their EHRs faster. The AMA toolkit for EHR transitions offers practical steps for any health care organization making this move.
For a real-world example of how community networks are adopting new models, check out our article on digital health in family practice reshaping community care in 2026. It shows how phased adoption and partnerships are closing the gap.
Want more practical strategies to navigate legacy health modernization? Subscribe to The Deep View Newsletter and get daily insights on what works in health tech.
Phased Modernization vs. Big Bang Overhauls
So which approach works best for legacy health systems like Texas Health or SSM Health?
The answer depends on your budget and risk tolerance.
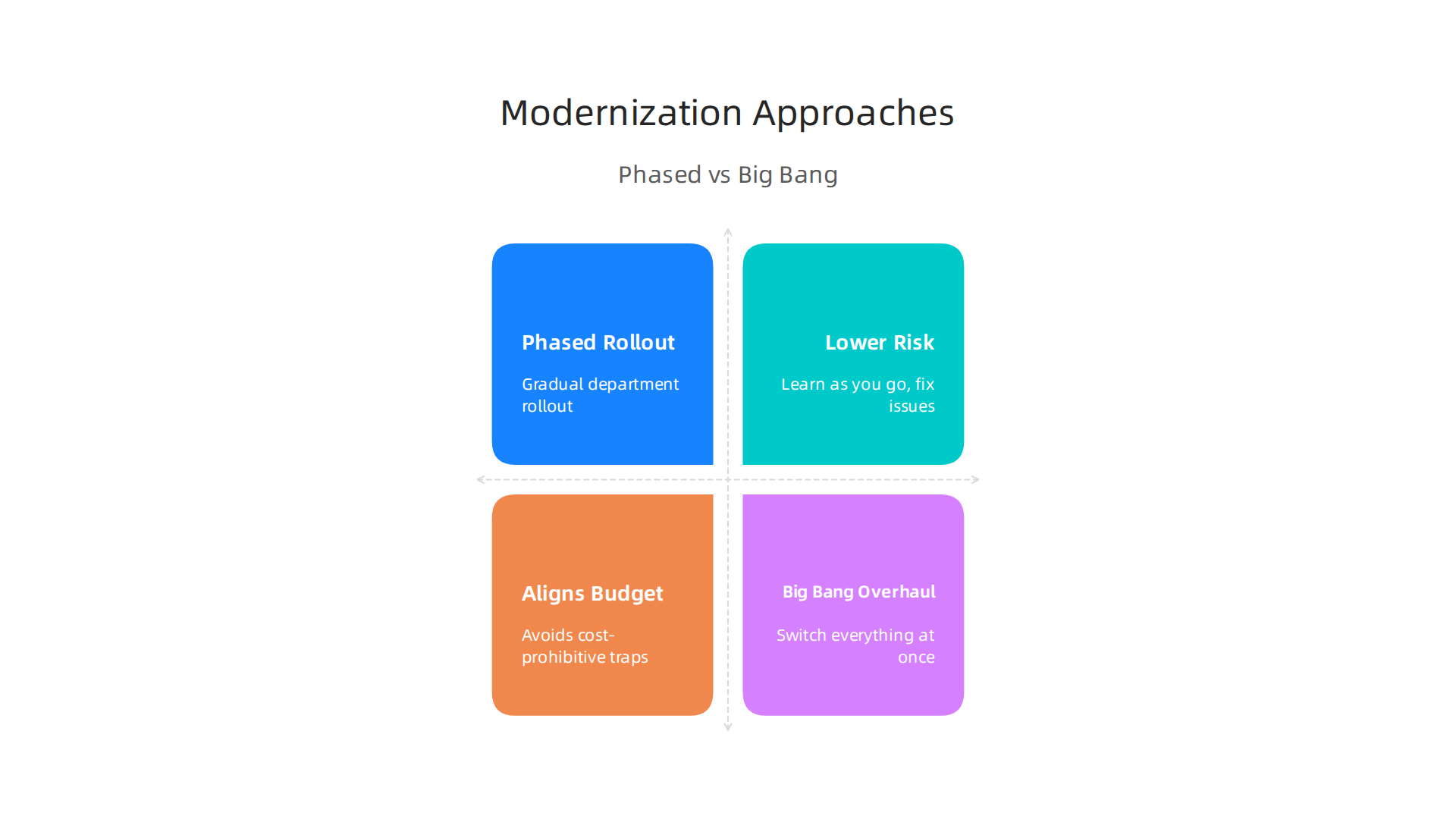
Phased modernization is the safer bet. You roll out changes gradually, one department or clinic at a time. This lets you keep operations running while your team learns the new system. The Black Book Market Research survey on rural hospital EHR replacement found that hospitals with limited budgets avoided the cost-prohibitive nature of legacy systems by taking it step by step. Phased approaches align with tight budgets and let you fix problems as they come up. No one gets shut down while you figure things out.
Big bang overhauls are the opposite. You switch everything at once. This can give you a faster transformation, but the risks are real. A single failure can stop all operations. The AMA toolkit for EHR transitions notes that big bang rollouts often lead to costly downtime and staff frustration. The 2026 HarmonyHIT market report on EHR migrations shows that 62% of hospitals rank EHR migrations as a top priority, but nearly 40% of hospital IT leaders still struggle with the stress of these large conversions.
For most legacy health organizations, phased modernization is the smarter move. You get the improvement without the heartache.
Curious how other health systems are making the shift? Read our article on clinical care technology innovations driving better outcomes to see phased approaches in action.
Want daily insights on what really works in health tech? Subscribe to The Deep View Newsletter and get clear, practical updates straight to your inbox.
Prioritizing High-Impact, Low-Risk Pilots
So you have chosen phased modernization. Smart move. But where exactly do you start? For a legacy health system like Texas Health or Banyan Health Systems, you do not try to fix everything at once.
You start with a high-impact, low-risk pilot.
Pick one area that truly matters. Revenue cycle management is a great place to begin. It directly affects your cash flow. Or choose a specific clinical workflow that frustrates your staff every day. Keep the scope tight.
This is exactly what the hospitals in the Black Book Market Research survey on rural hospital EHR replacement did. They tested the water in a small area first. This helped them avoid the cost-prohibitive traps that come with full legacy overhauls.
A focused pilot delivers quick wins. Bills get out the door faster. A nurse saves minutes on data entry. These small victories build trust and momentum.
But the real magic is in the data. You can measure exactly how much time you saved. You can track error reduction. This hard evidence builds your case for scaling up. The AMA toolkit for EHR transitions recommends collecting this KPI data before expanding. And Deloitte’s framework on measuring digital transformation ROI in health care shows that tracking these specific outcomes is how you secure budget for the next phase.
Think of it as proving your success before you ask for more resources.
For a real world example, look at how piloting automation in prior authorization or claims processing is changing the game. Read our coverage on why 94% of health plans are adopting AI in health insurance in 2026.
Want more practical strategies on what actually works in health tech transformation? Subscribe to The Deep View Newsletter and get clear, daily insights delivered to your inbox.
The Role of AI and Interoperability Standards in Unlocking Legacy Data
Once your pilot is running, a bigger question appears. How do you access the valuable data trapped inside your legacy health systems? You do not need to rip them out. Two tools can help: AI and interoperability standards like FHIR.
Think of legacy data as a giant filing cabinet. AI acts like a smart assistant who reads every paper in that cabinet. It finds patterns and extracts insights without replacing the cabinet. This means you get value from old data right away.
But AI needs data to work with. That is where FHIR APIs come in. FHIR (Fast Healthcare Interoperability Resources) is a modern standard for sharing health data. As the FHIR Ecosystem page explains, these standards help break down data silos.
By adding FHIR APIs on top of your old system, you create a bridge. New applications can talk to old databases. A 2026 HL7 blog post notes the industry is moving from planning to active implementation. This matters for legacy health organizations.
Data lakes help too. You copy data into a central lake using FHIR APIs. Then AI analyzes it for clinical decision support and population health insights. This enables real-time data exchange between old and new systems.
For example, a system like Texas Health, SSM Health, or Banyan Health Systems could use FHIR APIs to connect their legacy EHR with a new analytics platform. Doctors get real-time alerts about patient risks. Administrators see revenue cycle trends instantly.
The IntuitionLabs article on FHIR adoption reports over 90% of U.S. hospitals use FHIR. A PMC study on interoperable health systems shows how FHIR enables seamless integration. The tools are ready.
Want to see how these technologies improve care? Read our coverage on clinical care technology innovations.
For daily insights on AI and health tech, subscribe to The Deep View Newsletter.
FHIR APIs and Data Lakes
So you have added FHIR APIs to your legacy health system. Now what? Two big benefits show up fast: lower costs and better data access.
FHIR-based interfaces cut integration costs. Instead of building custom connections for every new app, you use one standard. That saves money and time. It also stops vendor lock-in. You are no longer stuck with one EHR vendor. As Firely explains, providers want independence, and FHIR gives you control over your own data.
Now about data lakes. Think of a data lake as a central pool. You copy data from your legacy system and your new apps into this pool using FHIR APIs. A PMC study shows how FHIR-based integration enables seamless data flow across different systems. Once the data is in the lake, you can run analytics on everything together. You can spot trends, track population health, and improve clinical decisions.
This matters for organizations like Texas Health, SSM Health, or Banyan Health Systems. Instead of leaving old data in the dark, you light it up. Your doctors get real-time insights. Your administrators see the full picture.
The FHIR Ecosystem page confirms that FHIR standards help break down data silos. In 2026, the tools are ready and proven.
Want to see more about how modern data systems improve care? Read about innovative primary care tech for senior care.
For daily insights on AI and health tech, subscribe to The Deep View Newsletter.
AI for Clinical Decision Support
Once you’ve got that data lake humming, the next natural step is letting AI do the heavy lifting. Here is where your modernized legacy health system really starts paying off.
AI algorithms can now run on top of your existing legacy data. They scan for things humans might miss. Drug interactions. Sepsis risk. Deteriorating patient vitals. The system flags these in real time. That means your doctors get early warnings before a crisis hits.
The beauty of running AI on a modernized data layer is that you don’t need to rip out your old EHR. You just add an AI layer on top. As the HL7 blog notes, 2026 is the year healthcare moves from planning to active implementation of standardized data exchange. The data is ready. The AI is ready.
What matters most is choosing a vendor-neutral AI platform. These tools work across systems from Texas Health, SSM Health, or Banyan Health Systems without custom integrations. That minimizes disruption and accelerates time-to-value. You get the insights fast without a long implementation project.
Want to see how this plays out in practice? Read about digital health in family practice to understand how community clinics are improving clinical decisions with AI.
For daily updates on these AI-driven health trends, subscribe to The Deep View Newsletter.
Building a Business Case for Adoption: From Cost to Value
So you have seen how AI can transform clinical decisions on top of your legacy health data. Now comes the harder part. Getting leadership to greenlight the investment. Here is what works in 2026.
A strong business case moves beyond simple ROI. It includes quality improvements, patient satisfaction, and competitive advantage. The old way only looked at cost savings. But that misses the bigger picture. A survey found that fewer than 30% of health system leaders reported significant ROI from virtual care. Why? Because traditional metrics miss the real value. As experts at Smart Health Asia explain, using the right KPI framework helps you capture the full value of digital health investments.
Think about this. Fewer medication errors. Faster diagnoses. Lower readmission rates. These are the outcomes that matter to patients and payers alike. And they are the outcomes that build a convincing business case. As Deloitte’s framework for measuring digital transformation ROI shows, the smartest organizations quantify both financial and clinical returns. The conversation shifts from "how much does this cost?" to "how much value does this create?"
A visual timeline helps too. Show stakeholders the value trajectory over 12, 24, and 36 months. Start with quick wins like reduced alert fatigue and staff satisfaction. Move to medium-term gains like improved patient throughput and lower complication rates. End with long-term competitive advantage in your market.
For regional systems like Texas Health, SSM Health, and Banyan Health Systems, funding is more accessible than you think. Grants support digital health modernization. Value-based care incentives reward better outcomes at lower cost. Vendor partnerships can offset upfront expenses. You do not need a massive budget. You need a clear plan tied to measurable outcomes that your board can track.
Want to see how other systems are making the case for innovation? Check out how clinical care technology innovations drive better outcomes in palliative and dementia care.
For daily updates on health tech trends and the AI tools shaping care delivery in 2026, subscribe to The Deep View Newsletter.
Best Practices for Change Management and Stakeholder Alignment
Building a solid business case is one thing. Getting your team on board is another. Change management in healthcare is hard. Really hard. But the systems that do it well share some common habits.
Here is what works in 2026.
Engage clinicians and administrators early. Do not wait until the contract is signed. Bring nurses, doctors, and IT leaders into the conversation from day one. When people help shape the solution, they own it. The Clinical Transformation in Technology framework shows that harvesting learnings from successful implementations early on builds momentum. Let your skeptics become your champions. It works.
Build structured training programs. Vague promises like "we will figure it out as we go" create resistance. Instead, create clear training paths. Hands-on workshops. Sandbox environments. Peer mentoring. Change management in healthcare succeeds when people feel confident using the new tools. A practical guide on healthcare change management explains that training reduces fear and accelerates adoption. Your staff will thank you.
Communicate constantly and visibly. Leaders need to show up. Not just in email announcements. In huddles. In hallways. In video messages. Talk about the "why" behind the change. Share early wins. Be honest about struggles. The 2026 healthcare trends report emphasizes keeping technology human centered and addressing change fatigue head on. Your team needs to hear from you regularly.
Organizations like Texas Health, SSM Health, and Banyan Health Systems are using these practices to modernize their legacy health systems. They are not perfect. But they keep communicating, keep training, and keep listening.
The result? Faster adoption. Better patient outcomes. And a culture that welcomes innovation instead of fighting it.
Engaging Clinicians from Day One
Getting your clinical team involved early is one of the smartest moves you can make when modernizing your legacy health systems.

Here is why.
Clinician champions can peer-educate and address concerns in real time. Doctors and nurses trust their peers more than they trust an announcement from the C-suite. A nurse who has used the new system on a shift can answer questions from a skeptical colleague in the hallway. That kind of real time coaching builds confidence fast. The Clinical Transformation in Technology framework shows that harvesting lessons from successful implementations early on creates momentum. Let your skeptics become your champions.
Involving end users in selection and customization improves satisfaction. When you let the people doing the actual work help choose the tools, you get higher adoption. A nurse knows which charting fields matter most. A doctor knows which alerts cause alert fatigue. A practical guide on change management in healthcare explains that participation reduces fear and speeds up adoption. Organizations like Texas Health, SSM Health, and Banyan Health Systems have seen this play out in real time.
Want to see how digital tools are reshaping daily clinical work? Check out how digital health in family practice 2026 reshapes community care.
And if you want fresh insights on AI and tech trends in healthcare delivered daily, the The Deep View Newsletter is the resource you need.
Training and Continuous Education
Getting clinicians on board early is only the first step. The next challenge is making sure they actually know how to use the new tools. That is where training and continuous education come in.
Just-in-time training works better than one-size-fits-all sessions. When training happens right when someone needs it, retention goes way up. A nurse switching shifts can watch a quick video on the new charting process before they start. A doctor can review one specific module before their next patient comes in. Instead of overwhelming everyone with everything at once, role-specific modules let each person learn what matters most to their job. Supporting a culture of change around a common vision helps sustain momentum, and the same logic applies to training.
Ongoing support keeps adoption strong after launch. Training cannot be a one-time event. Without continuous education, old habits creep back in and clinicians start avoiding the new system. Ongoing support like refresher courses, Q&A sessions, and access to a help desk ensures people stay confident and competent. Practices that focus on long term support see much better outcomes and avoid the costly cycle of retraining from scratch.
Linking continuous education with AI adoption can be powerful too. Learn how AI is reshaping health insurance in 2026 and how training plays a role in those changes.
For daily updates on AI and tech trends that can help you build a smarter training strategy, subscribe to The Deep View Newsletter.
Case Study Spotlight: Success Stories from Regional Health Systems
Training and continuous education set the stage. But the real proof comes from regional health systems that have already made the leap. Their stories show what is possible when you modernize with purpose.
Take a look at how systems like Texas Health and SSM Health are tackling legacy health infrastructure. These organizations moved away from clunky, outdated platforms and adopted modern, interoperable systems. For example, using HL7 FHIR standards helped them break down data silos and share patient information across departments and even with outside providers. This is a big deal because, by 2026, most successful systems are leaning heavily on standards like FHIR to drive real change, as noted by the HL7 blog on FHIR adoption.
The results? Key metrics tell the story:
- Reduced hospital readmissions: Better data flow means care teams see the full picture.
- Improved patient throughput: Less time wrestling with old software.
- Real cost savings: Money saved on inefficiencies and errors.
Banyan Health Systems is another great example. They focused on iterative deployment. Instead of a huge, scary rollout, they launched small changes one at a time. This let clinicians learn as they went, just like we talked about with just-in-time training. Their experience matches what the HIMSS report on closing the technology gap highlights: a phased approach works best for adoption.
What did these systems all share? Two big lessons stand out.
First, executive support was non-negotiable. Leaders backed the project publicly and privately. They gave teams the resources and air cover to try new things.
Second, they used an iterative approach. They tested, learned, and adjusted. This flexibility is key when moving off legacy health systems.
Want to learn more about how technology is reshaping specific regions? Check out our guide on Texas Medical Board regulations for health tech to see how local rules play into modernization.
For daily insights on the tech trends driving these success stories, subscribe to The Deep View Newsletter.
Summary
This article outlines a practical roadmap for regional health systems stuck on legacy technology, explaining why outdated, siloed systems harm care, security, and staff morale. It summarizes the main barriers—interoperability gaps, tight budgets, and cultural resistance—and shows how organizations can move forward without risking operations or blowing budgets. You’ll learn how to prioritize high‑impact pilots, build a business case that ties clinical outcomes to financial value, and choose phased modernization over risky big‑bang rollouts. The piece explains how FHIR APIs, data lakes, and vendor‑neutral AI layers can unlock trapped data, and it lays out concrete change‑management, training, and clinician engagement practices that improve adoption. By the end, readers will have action steps to start small, measure wins, secure funding, and scale transformation across their system.