
Introduction: Rethinking the Care Continuum
Picture this: You leave the hospital after a surgery, get handed a stack of papers, and are told to follow up with your primary care doctor.

But nobody calls that doctor. Nobody explains your new medicines. Within a week, you are back in the emergency room. Sound familiar? That is a failed transition of care.
Transitions of care simply mean the movement of patients from one healthcare setting to another. This could be from a hospital to a nursing home, from a specialist to your regular doctor, or from a clinic back to your home. The Joint Commission defines it as “the movement of patients between health care practitioners, settings, and home, as their conditions and care needs change” Care Transitions – Making Healthcare Safer III. When these handoffs are sloppy, patients fall through the cracks. Readmission rates spike, costs balloon, and safety takes a hit. That is why improving how we manage these moments has become a top priority for health systems, insurers, and technology companies.
For too long, healthcare has been a series of disconnected episodes. You see a specialist, then you see a different specialist, and nobody talks to each other. But in 2026, the old model is crumbling. A new, continuous approach is emerging. We now have digital tools that share records in real time, AI that flags high-risk patients before they leave the hospital, and care teams that span both virtual and in-person visits. These innovations are making care access easier and primary care services more connected. They help with everything from long term care follow-ups to medication management.
This article explores the latest technological, regulatory, and strategic developments shaping transitions of care in 2026. We will look at data, expert perspectives, and real-world examples to show you what is working. If you are a healthcare leader, a healthtech founder, or a clinician looking to improve patient outcomes, this guide is for you.
Want to stay ahead of the fast-moving changes in healthcare technology? Get clear daily AI updates from The Deep View Newsletter and never miss a critical trend.
Defining Transitions of Care in 2026
So what exactly are these transitions we keep hearing about? In simple terms, the classic definition hasn’t changed much. The Joint Commission defines transitions of care as “the movement of patients between health care practitioners, settings, and home, as their conditions and care needs change” Care Transitions – Making Healthcare Safer III. That covers everything from a hospital discharge to a move from a nursing home back to your house, or even a routine referral to a specialist.
But here is the 2026 twist. The term has grown to include digital handoffs, telehealth visits, and the coordination between virtual and in-person care teams.

A patient now might start with a video consult, get lab work done at a retail clinic, see a specialist remotely, and then have follow-up messages from their primary care services provider. Each handoff in that chain is a transition, and if any link breaks, the whole thing falls apart. That is why groups like the American Case Management Association have published official standards to define what high-quality transitional care really looks like.
Having a shared definition matters. Without it, you cannot measure whether a transition was smooth or messy. You cannot track improvements in care access or long term care follow-ups. And you definitely cannot hold anyone accountable. That is why organizations like NCQA measure transitions of care as a key quality metric, tracking things like whether a patient received timely follow-up after discharge
Transitions of Care (TRC) – NCQA. This foundation helps health systems focus their technology in healthcare investments on the handoffs that matter most.
For a deeper look at how primary care services are adapting to these connected models, check out our guide on innovative primary care tech and models reshaping senior care in 2026.
The Shift from Acute to Continuous Care
One big reason transitions of care are changing in 2026 is the move to value-based care. Instead of paying for each episode, providers earn rewards for keeping patients healthy over time. This pushes care access and long term care to be connected. Technology in healthcare enables continuous monitoring and proactive outreach. Wearables and remote tools help primary care services catch problems early, reducing the need for acute transitions. As experts note, a strong focus on transitions of care supports both patients and physicians AJMC. To learn more, see how clinical care technology innovations are reshaping care continuity.
Key Technologies Reshaping Care Transitions
So, what tools are actually making transitions of care better in 2026? A few powerful technologies lead the way.
First, AI and predictive analytics help care teams spot high-risk patients before problems start. These systems analyze patient data to personalize transition plans and prevent readmissions. The AI-Based Care Coordination Market is now worth USD 2.15 billion in 2026 according to industry analysis. Hospitals already use predictive analytics to identify patients who might need extra support after discharge, cutting down on unplanned returns as MGH IHP researchers found.
Second, interoperability standards like FHIR are solving the old problem of systems that could not talk to each other. AI now helps structure messy data during health information exchanges, making records usable across different providers IntuitionLabs explains this shift. This means a primary care services team gets real time updates from the hospital, no fax machine required.
Third, blockchain technology is being piloted for secure health records during handoffs. It creates a verifiable log of who accessed data, adding trust to every transition.
These tools all work together to improve care access and long term care coordination. For leaders looking to modernize their approach, learn how innovative primary care tech and models are reshaping senior care in 2026.
Staying current with this fast moving technology is hard. That is why thousands of health leaders read The Deep View Newsletter each morning for clear AI updates you can actually use.
AI and Predictive Analytics
Which patients will struggle after leaving the hospital? AI now helps answer that question before they walk out the door.
Machine learning models train on electronic health record data to forecast which patients are likely to face complicated recoveries. This lets care teams personalize the discharge plan from day one, improving care access and follow up.
Natural language processing, a type of AI, reads clinical notes to find social factors. Things like whether a patient has family support or reliable transport. These details often make or break a long term care plan.
The results speak for themselves. A study on AI based clinical decision support systems showed they help catch risks early and prevent unplanned returns to the hospital according to researchers. Another analysis showed predictive analytics can directly improve outcomes in primary care services as MGH IHP researchers reported.
For health leaders looking to apply this in their own organizations, see how digital health in family practice 2026 reshapes community care.
Keeping up with fast moving AI tools is hard. Stay informed with clear, daily updates that actually help your work. Read The Deep View Newsletter each morning.
Interoperability and FHIR Standards
AI is only as smart as the data it can access. And too often, data gets stuck in silos between your primary care services and the hospital.
That is where FHIR standards come in. FHIR (Fast Healthcare Interoperability Resources) APIs act like universal translators. They allow a hospital, a clinic, and your own health app to share information securely. This opens up real care access across the whole system. According to a recent look at health information exchange, these standards are the backbone of modern data sharing according to analysis from IntuitionLabs.
The 2024 ONC Cures Act Final Rule pushed FHIR adoption forward, but disparities remain. Many smaller facilities still struggle to keep up. For health systems looking to close this gap, learning how to modernize legacy health systems is a critical first step.
When FHIR works well, the results for transitions of care are powerful. One case study showed real-time medication reconciliation across settings reduced adverse drug events by 40%. This makes a huge difference for patients moving into long term care or back home.
Better data flow turns technology in healthcare from disconnected tools into a single, helpful network.
Access as the Foundation of Seamless Transitions
Good data sharing gets information where it needs to go. But even the best FHIR setup falls flat if patients cannot actually reach care after leaving the hospital. That is why care access is the true starting point for smooth transitions of care.
Think about it. A patient leaves the hospital and needs a follow up with their primary care services. If they cannot get an appointment, or they have no way to talk to a nurse, they end up back in the ER. The fix? Health systems are now embedding transition navigators and community health workers to bridge those gaps.
Digital tools also play a huge role. Remote patient monitoring and telehealth follow ups give patients a lifeline after discharge. One study found that telemedicine patients were 76% less likely to be readmitted within six months compared to those who did not use it according to research from HealthViewX. Another study showed that home digital monitoring significantly cut hospitalizations and ER visits over six months according to a study in PMC.
But here is the challenge. These access tools must work for everyone, including people with low digital literacy. A fancy app does no good if a patient cannot use it. The best technology in healthcare is the kind that actually meets people where they are.
Want to see how home based digital health platforms are creating real access today? Check out our look at how these tools are transforming healthcare in 2026.
Telehealth and Remote Patient Monitoring
So how do health systems turn better care access into reality after discharge? Two tools lead the way: telehealth visits and remote patient monitoring (RPM).
Post-discharge telehealth follow ups are now standard for many conditions. One study found that telemedicine patients were 76% less likely to be readmitted within six months
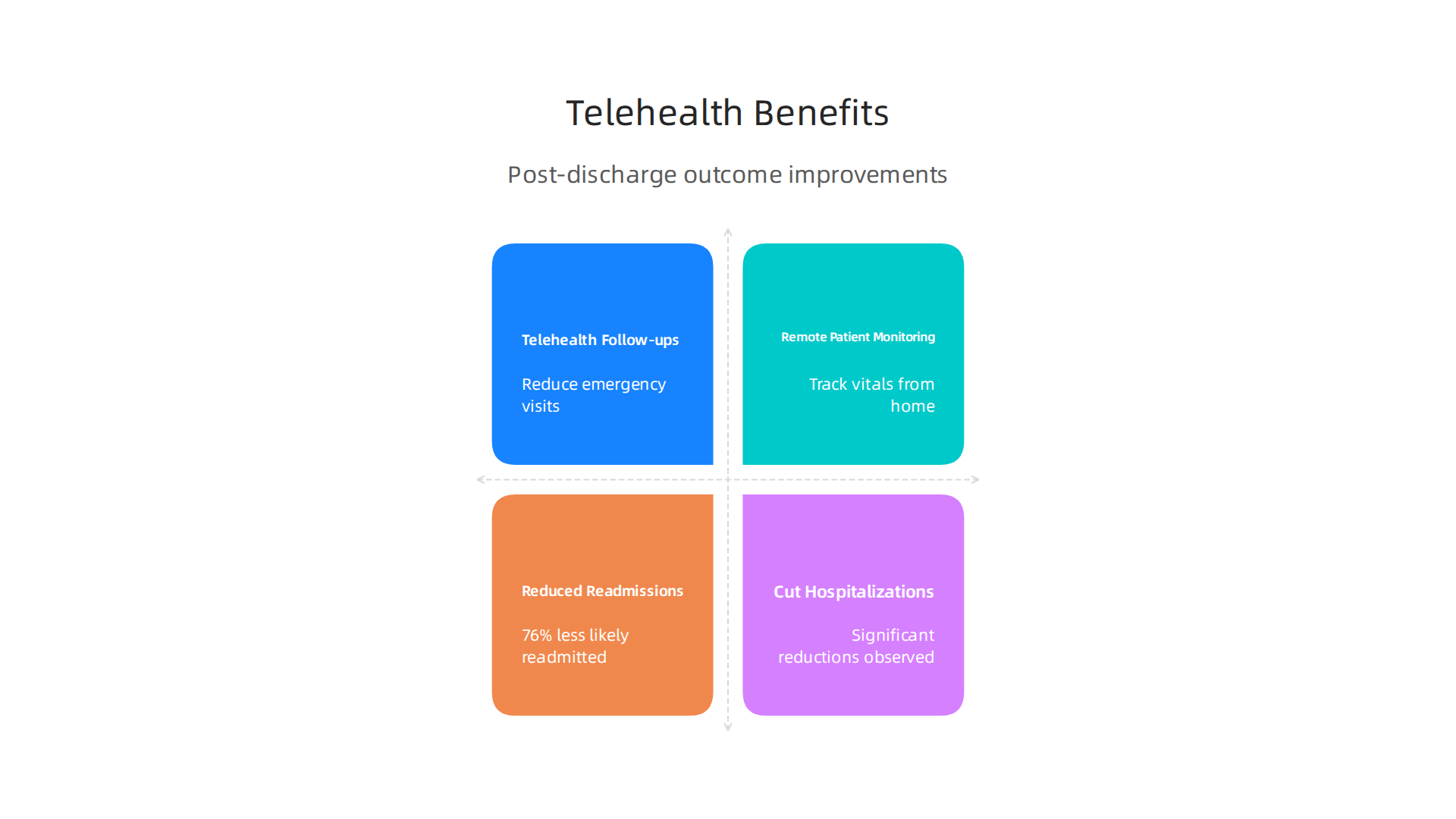
according to HealthViewX. This alone keeps unnecessary emergency department visits down.
Remote patient monitoring takes things a step further. RPM devices track vital signs like blood pressure or oxygen levels from home.

If something changes, the system alerts providers right away. Another study found that home digital monitoring significantly cut hospitalizations and ER visits over six months according to research in PMC.
Policy changes in 2025 and 2026 helped speed up this shift. Medicare expanded reimbursement for RPM, making it easier for hospitals to invest in this technology in healthcare. Patients now get connected monitoring as part of their long term care plan. This turns a single hospital visit into a smooth transitions of care experience.
Want to see how these tools change outcomes for specific groups? Check out how innovative primary care tech is reshaping senior care in 2026.
Innovation in Care Coordination Platforms
Telehealth and RPM generate a lot of data. The challenge is making sense of it all. That is where care coordination platforms come in.
These integrated platforms pull data from hospitals, clinics, labs, and home devices into one shared care plan. Every provider sees the same information. This reduces confusion during transitions of care and helps teams work together on primary care services and long term care goals.
AI makes these platforms smarter. In 2026, the AI-based care coordination market reached $2.15 billion and continues growing fast according to Mordor Intelligence. These tools use predictive analytics to flag issues like missed medications or pending referrals before they cause problems. One study found that AI-based clinical decision support can reduce unplanned hospital readmissions per research in PMC.
Here is the catch though. Platforms only work if clinicians actually use them. Tools that add extra clicks or slow down workflows fail fast. The best platforms fit into existing routines and reduce burden instead of adding to it.
If you want to see how modern technology in healthcare improves care access across different settings, check out our guide to modernizing legacy health systems in regional hospitals.
Want to stay ahead of innovations like these? Subscribe to The Deep View Newsletter for clear daily AI updates that help you make smarter decisions.
Case Studies of Effective Transitions
Real examples show how combining people and tech improves transitions of care and cuts costs.
-
Health System A rolled out a digital discharge checklist for heart failure patients. The tool reminded clinicians to check key steps like medication changes and follow-up appointments. Result: readmissions dropped by 25%. Research on remote health monitoring supports this kind of approach, showing home monitoring can significantly reduce hospital stays per a study in PMC.
-
Health System B paired community paramedics with telehealth. After discharge, paramedics visited patients at home and connected them remotely to a nurse. This cut ER visits by 30%. One study found that telemedicine patients were 76% less likely to be readmitted within six months according to HealthViewX.
What makes these programs work? It is not just the technology. It is the human touch. The digital tools guide the team, but the paramedics, nurses, and doctors build trust with patients. This hybrid model blends primary care services with technology in healthcare to improve care access.
If you want to see how similar hybrid models support long term care, read our article on digital health in family practice 2026 reshapes community care.
Regulatory and Compliance Landscape
The examples we just covered show how strong transitions of care programs can really work. But here is the thing. Keeping those programs running safely and legally takes serious attention to rules and regulations. The landscape changed a lot in 2026, and it keeps evolving.
If you are building or managing a transition program, you need to know three big regulatory shifts happening right now.
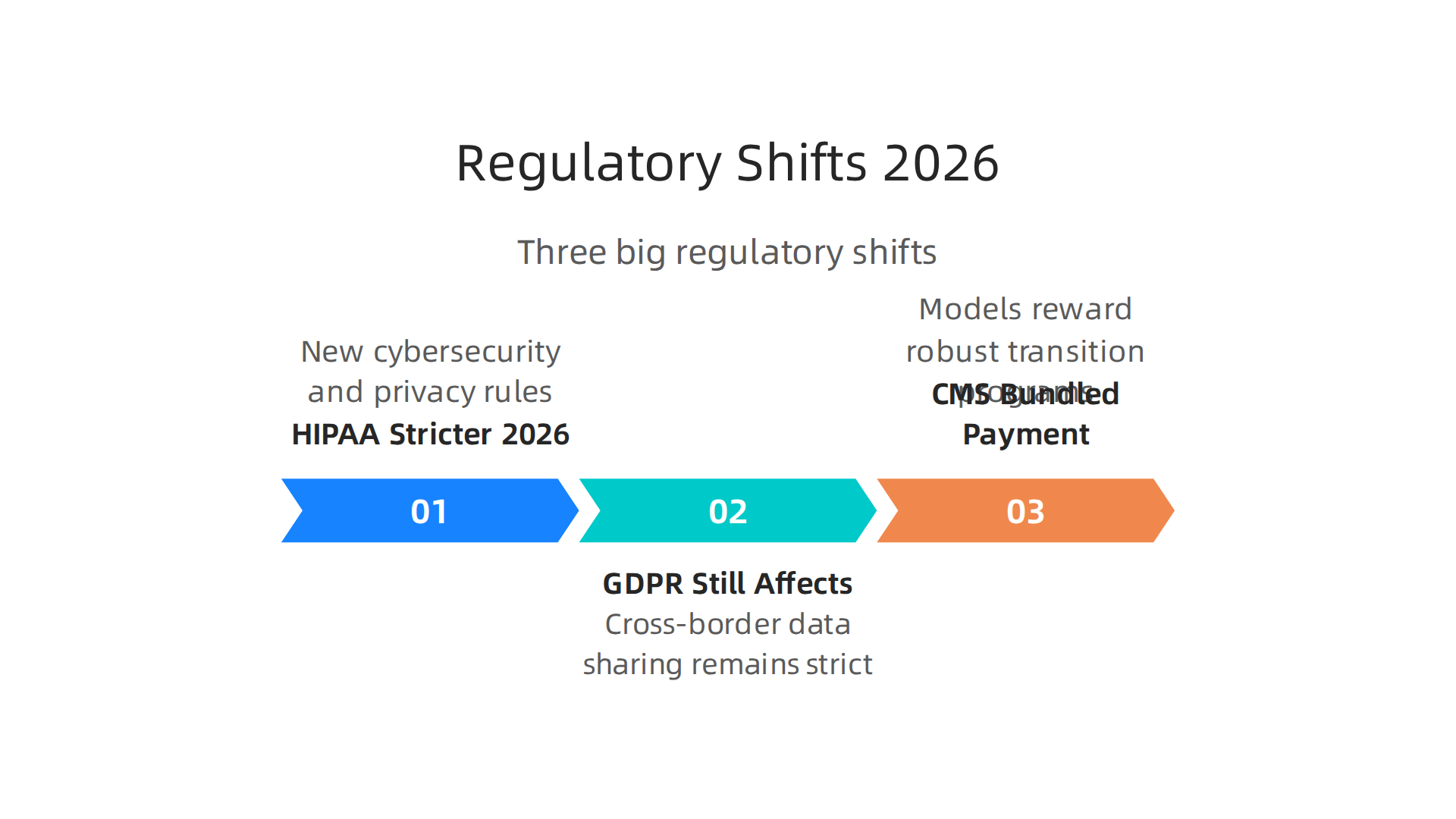
HIPAA Gets Stricter in 2026
The biggest update is to HIPAA. New rules came into effect in 2026 that directly affect how you share patient data during transitions of care. A major HIPAA Security Rule update introduced new cybersecurity requirements and stricter compliance standards per BARR Advisory. The deadline to update your Notice of Privacy Practices passed on February 16, 2026, and covered entities had to make major changes to reflect new federal privacy requirements according to Buchalter.
What does this mean for you? Stricter penalties for breaches. And stricter privacy protections for sensitive health data, including reproductive and behavioral health information as covered by Chess Health Solutions. If your technology in healthcare platform shares patient data across care settings, your compliance team needs to double check every data flow.
GDPR Still Affects Cross-Border Care
If your transitions of care program touches patients in the EU or partners with European providers, GDPR still applies. The rules around cross-border data sharing remain strict. For digital health platforms coordinating care access internationally, you need clear consent mechanisms and data processing agreements in place.
CMS Bundled Payment Models Incentivize Better Transitions
Here is some good news. The Centers for Medicare and Medicaid Services (CMS) introduced new bundled payment models in 2026 that directly reward robust transition programs. These models link payment to outcomes like reduced readmissions and better patient follow through. That means strong primary care services and coordinated long term care after discharge now have a clearer financial upside.
The takeaway? Compliance is not just a burden. Doing it right protects your patients, your reputation, and your bottom line.
For a deeper look at how modernizing your health systems can help meet these regulatory demands, read our guide on how to modernize legacy health systems in regional hospitals.
Strategic Implications for Healthcare Leaders
All those new rules we just talked about? They are not just paperwork. They send a clear signal. Healthcare leaders who treat transitions of care as a side project are going to fall behind fast.

Here is what the landscape in 2026 means for your strategy.
Invest in Transition Infrastructure Now
Let’s be direct. Spending money on care coordination tools and staff is not optional anymore. It is a strategic must. Why? Because it directly lowers your total cost of care and improves patient outcomes. The McKinsey report on the future of US healthcare makes it clear that economic pressure will keep squeezing margins through at least 2027 as outlined by McKinsey. Every readmission you avoid and every smooth handoff you create saves real dollars.
And it is not just about money. Better transitions of care mean better care access for your patients. When you invest in the right infrastructure, patients do not fall through the cracks between the hospital and their follow up primary care services or long term care plan.
Balance Technology Adoption with People
Here is the thing that trips up a lot of leaders. You can buy the best software in the world for technology in healthcare. But if your nurses and care coordinators do not know how to use it, or worse, if they resent it because it was forced on them without training, you will get mediocre results.
The other side of this coin is workforce training and change management. We are already looking at a projected shortage of about 100,000 critical health care workers by 2028, according to the American Hospital Association as reported by AHA. You cannot afford to lose more staff because of clunky tech rollouts.
So invest in training first. Make sure your teams understand the "why" behind the new tools. When they see how a platform helps them coordinate care access more easily, you get buy in.
Build Real Partnerships
No health system can go it alone anymore. The best transitions of care programs in 2026 rely on partnerships. Think about it. You need your hospital to talk to community clinics. You need your primary care services providers to talk to skilled nursing facilities. And you need tech vendors who understand the whole picture.
The PMC analysis on the future of healthcare highlights that digital transformation and interoperable data are at the top of the list for what matters next per PMC. That means partnerships between health systems, tech vendors, and community organizations are not just nice to have. They are how you scale.
For example, the shift toward home based care is one of those partnership opportunities. If you are thinking about how to expand long term care into the home, consider the innovations happening in senior care. Our guide on innovative primary care tech and models reshaping senior care in 2026 shows exactly how these partnerships can work.
The Bottom Line for Leaders
Here is your takeaway. Compliance is the floor. Strategy is the ceiling. Use the regulatory pressure as a reason to finally build the transition programs you have always wanted. Invest in your infrastructure. Train your people. And partner smartly. Your patients and your bottom line will thank you.
Future Outlook: Toward an Integrated Continuum
So where is all this headed? By 2030, transitions of care could feel almost invisible to patients. Imagine a system where predictive AI and real time data flow automatically coordinate your next step. You leave the hospital, and your follow up with primary care services is already scheduled. Your long term care plan adjusts based on your recovery at home. The handoff happens behind the scenes. Experts at Provista predict that by 2030, technology will finally stitch together these disconnected pieces as noted by Provista.
But the road to that seamless future has real bumps. Equity is a big one. Not every patient has equal care access to the internet or a smartphone. Privacy concerns around sharing health data across different systems are still unresolved. And interoperability? Different hospitals, clinics, and long term care facilities still use software that does not talk to each other well. The PMC analysis highlights that digital transformation and interoperable data are top priorities, but we have not cracked the code yet per PMC.
The organizations that win will be the ones that build trust. That means being transparent about how AI makes decisions. It means designing tools that clinicians actually find helpful, not frustrating. And it means putting the patient experience at the center, not just the technology. If you want to see what an integrated continuum looks like in practice today, check out how innovative primary care tech and models are reshaping senior care in 2026 here.
Staying ahead of these shifts requires staying informed. That is why we recommend The Deep View Newsletter. It delivers clear daily updates on AI and technology trends that are shaping healthcare subscribe now. Do not let the future catch you off guard.
Summary
This article explains how transitions of care — the handoffs between hospitals, clinics, home, and long‑term care — are evolving in 2026 and why getting them right matters for patient safety, cost control, and quality metrics. It reviews the key technologies reshaping handoffs, including AI/predictive analytics, FHIR interoperability, blockchain pilots, telehealth, and remote patient monitoring, and shows how those tools combine with people‑centered roles like navigators and community paramedics. The guide covers operational lessons from case studies, explains regulatory changes (notably tighter 2026 HIPAA rules, GDPR implications, and new CMS bundled payments), and outlines strategic priorities for leaders: invest in infrastructure, balance tech with training, and build partnerships. Readers will learn practical ways to reduce readmissions, improve follow‑up access, and design care coordination systems clinicians will actually use while staying compliant and equitable. The article also highlights gaps — digital equity, interoperability challenges, and workforce strain — and points toward a 2030 vision of nearly invisible, automated handoffs that keep patients on track.